How is it already mid-February? I swear each year flies by faster and faster... and yes, I realize that's a cliche thing to say. I did some really fun volunteering earlier this month that took up my usual blogging hours, so I'm long overdue for a post today. I'll be writing about those experiences soon, but today I've got a Book Alert on the
Graded Motor Imagery Handbook, by Lorimer Moseley, David Butler, and their crew with the
NOI Group. The NOI Group is the Neuro Orthopedic Institute of Australasia that teaches a variety of topics related to neuroscience and pain. I've previously written about their books
Explain Pain and Explain Pain Supercharged as well as my experience meeting Lorimer Moseley
here. You might call me a NOI Group Superfan at this point since I think I've read all their books, but not their research articles because there are hundreds of those. Working on it. This topic was fueled by my work with the Seattle Children's Hospital Pain Management Team, and every time I read one thing, I identify tons more to learn about. Definitely falling down the chronic pain rabbit hole over here.
The Graded Motor Imagery (GMI) Handbook was on my
list of six books I wanted to read in 2020 which I'm tracking on the right side of the blog for the year. One down, five more to go! Now that I've read it, I've already started incorporating the concepts into practice, and if you're a physical therapist, I highly recommend you read this, particularly if you treat patients experiencing chronic pain or CRPS, but also this probably should be considered with more of our patients. This topic, as are all the topics that come from the NOI Group, is complicated, so I'm trying to share my understanding of what I read.
I've chosen one example to use to demonstrate the concepts of GMI throughout this post. GMI can be applied to injuries anywhere in the body, though. I've used it more in extremities than in the spine, but I also don't treat many patients with chronic neck or back pain in the clinic. Let's say you sprained your left ankle playing soccer yesterday. It hurts. You've just injured it! It is reasonable to have pain right now and the amount of pain seems appropriate based on the mechanism you experienced. Tissues may have some damage - maybe your anterior talofibular ligament has a few fibers that were damaged. This is the most commonly injured ligament in an ankle sprain and you've probably already hurt it before if you're playing soccer. Maybe you see some bruising, swelling, and are having a little difficulty walking. The XRAY says you didn't break anything. The doctor at urgent care puts you in a boot and tells you that you can do as much activity as you can tolerate and that you can wean out of the boot in a week or two.
In this acute phase of a recent injury, your brain is processing many inputs from your injured ankle and it does so in the "typical" way. The brain processes the sensory inputs from the ground and the boot and produces your pain experience. Maybe you don't have much pain because the injury has occurred and ended, no additional threat is perceived, and you know that you've had this experience before and that things will recover quickly. You think you'll be ready for the soccer tournament next month without any issues. This is when you think, "phew, it's not broken and it's not really even hurting that much. I'll just wear this boot and be back to normal soon." You probably won't even see a physical therapist, though I've previously written
here why you should, even if it's just a minor ankle sprain.
But what happens if, for a variety of possible reason(s), the pain doesn't go away, or maybe even worsens. Your simple ankle sprain from playing soccer persists longer than you think it should. You find yourself unable to wean out of the boot after several weeks of wearing it and you've gone back to the doctor who does an MRI that says there's some mild damage but your pain level has remained higher than it should be. You've finally gone to your physical therapist and they have been able to get you walking a bit more, but you still can't really tolerate activities and pain is worse than what you expect. Maybe swelling persists and you're still having trouble walking a few weeks later. Sometimes you could even experience a cold, sweaty, purple foot with weird growth of your leg hair or toenails on that side. You've stopped playing soccer and are spending less time out with your friends because that's where you would typically see them. Maybe you've declined invitations to hike and are even losing sleep sometimes because your ankle hurts. Your job is being affected because your work requires you to stand for extended periods of time and you can't tolerate that because your ankle still hurts. All of this from a little ankle sprain that isn't healing the usual way.
The research in the GMI Handbook (of which there is A LOT) explains that people who experience chronic periods of pain sometimes lose their ability to differentiate between their right side and their left side. The brain is affected by your ankle injury. In some patients, you might even start feeling pain on the other ankle. If you're thinking what I was thinking when I first read about this, you might be thinking "No way!?!?!?! How?!?!" That's how I felt, at least.
Now that I've started using GMI assessments and treatment tools in the clinic, I can actually see that patients have difficulty doing this. I wouldn't have believed it if I hadn't seen it for my own eyes. Ive worked with patients, particularly with foot/ankle injuries, who haven't put their foot on the ground in months. MONTHS! They're spending time on crutches or even worse - in wheelchairs. They exhibit fear towards walking, standing, or even having their feet touched. The brain is processing input signals - maybe even caused by being in a boot - for far too long and starts to understand the input signals differently. Not only does your brain start to confuse things, but it also starts to react to stimuli in new ways. Things that wouldn't typically hurt most people, like the feeling of your sock on your ankle, now hurt. This is called
allodynia: a central pain sensitization in which neurons exhibit increased response to normally non-painful stimuli. Basically - you experience pain to a stimulus which typically would not be painful. I see allodynia frequently in the clinic and have actually experienced it for myself. About eight years ago, I badly cut my finger on one of those apple corer things while helping my sister cook Rosh Hashanah dinner for our family. Sometimes even now if I touch that old cut, I might feel a sharp pain and pull my hand away, but usually I don't even notice it. Patients who have had chronic pain sometimes cannot tolerate me touching their foot with my hands or even a towel because it feels too painful. They pull away or shout or cry or sometimes even kick me (unintentionally, I'm sure), and they recognize that their response to what I'm doing doesn't make sense.
Graded Motor Imagery is a tool to try to restore the brain's proper understanding of left versus right while exercising the brain. The book outlines a series of steps starting with understanding left versus right, followed by imagined movements where the patient concentrates on their injured ankle while mentally picturing themself doing activities like walking, followed by the use of mirror therapy to almost trick the brain into thinking that their injured limb is moving without pain while you're moving your non-injured limb while looking into a mirror.
 |
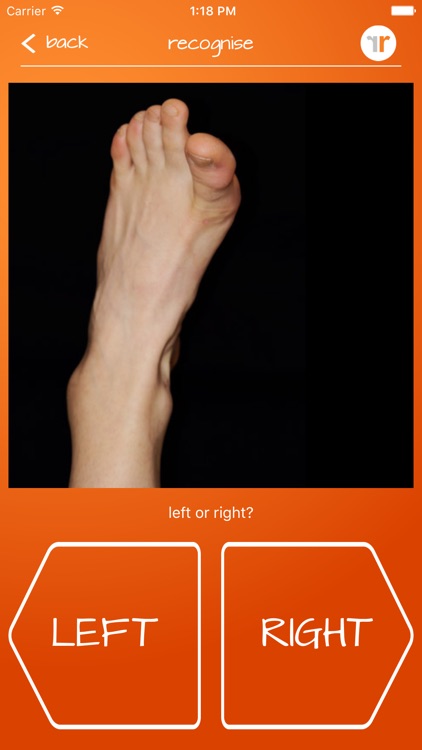
| From the Recognise App |
When I see a patient experiencing chronic pain of their ankle, I'm using an app created by the NOI Group called "Recognise Foot" (yes, spelled that way, because they're Australian and they don't like the letter Z). The app shows you pictures of a foot and you have to identify if it is a left or a right one. (They have apps for several different body parts). You can change the settings to start with fairly simple images like this one --> with a black background in typical positions to more complex images with varied backgrounds that are covered in paint or wearing a cast or flipped upside-down and it's basically like playing a game to see how fast you can identify the side of the body and how accurate you are. I've tested out the app for the hand (Recognise) and the app for the foot (Recognise Foot), each of which are $5.99 at the App Store.
A normal result would be at least 90% accuracy and symmetry between sides as well as response time of less than .2 seconds. The app will tell you your scores and you can use it to assess the patient's ability to discriminate between left and right as well as treat them using the app. I've been adding this as a home exercise program component to patients who have been experiencing chronic pain and having them "play the game" several times per day in addition to doing some activities to try to get them moving towards less pain.
A word of caution: the GMI Handbook does say that some people will experience pain just from using the app. This is not something I have experienced yet, but if it does occur, there are ways to change the settings on the app so the patient has more time to respond or less images. Also you can actually regress from this to watching other people move, focusing on the other person's body. For example if your ankle pain was increased just by using the app, you could go to the mall and watch people walking and focus on their ankle instead. There's science to support this regression and the book talks discovering this using monkeys who would watch people eat and some of their own brain cells that would be activated if they were eating would "light up" as if they were doing the activity themself. It's a less intense way for your brain to process information, watching someone else do an activity, because of the ways the sensory and motor cortexes of the brain are uniquely used with watching versus participating in activity.
Ultimately, GMI is a science that is still developing. There is research to support some of the claims, but not all of them and the NOI group points out where there are holes in the evidence. There is evidence to support using this treatment in specific patients, such as those with CRPS, and less evidence for others. Some of my colleagues are using this treatment more frequently and with patients in more acute pain states. Some colleagues don't use it because they don't know anything about it - like myself only a few months ago. The app is actually pretty fun and if you don't have pain doing it, who wouldn't benefit from some brain training? I'm tempted to see if the basketball players I work with have any change in their reaction time by using this sort of brain training to try to use if for performance enhancement, but again, I have no evidence to support that thought and can't usually use them as guinea pigs. I'm curious to know who else is using GMI in their clinical practice, how often, for what conditions, and what others have found with using it. And I highly recommend that PTs read this book to learn about where we are on this type of patient care right now and to see if it might help some of your patients.