 Today I'm writing about the CALU Summit which I recently attended virtually. The name CALU comes from the combination of Clinical Athlete and The Level Up Initiative. I've attended A LOT of continuing education courses over the past seven years as a PT and I'm certain this was the most fun learning I've ever experienced. This was my first CALU Summit - their second time holding the event - but I have interacted with both groups in different ways for many years. In the past, I went through the Level Up Initiative's mentorship program and then served as a mentor and am planning to again. I've previously written about them here. Clinical Athlete puts out podcast episodes that I've listened to and I've participated in some of their journal clubs. Both groups have loads of social media worth following and are led by super smart physical therapists who believe in educating healthcare providers. These two networks have impacted my patient care and helped me develop as a physical therapist. In my opinion, both groups are MUST FOLLOW accounts for physical therapists, strength coaches, athletic trainers, and any new grad healthcare provider - but would also be great options for sport coaches, athletes, and parents of athletes to check out! (Specific names to search for on Instagram include: @thelevelupinitiative @clinicalathlete @zakgabor.dpt @stephallen.dpt @quinn.henochdpt @jared.unbreakablestrength @rebuild_stronger - sorry if I missed anyone!) Here are some of my favorite take-aways from the Summit! (Disclaimer - this is what stood out to me, not direct quotations.)
Today I'm writing about the CALU Summit which I recently attended virtually. The name CALU comes from the combination of Clinical Athlete and The Level Up Initiative. I've attended A LOT of continuing education courses over the past seven years as a PT and I'm certain this was the most fun learning I've ever experienced. This was my first CALU Summit - their second time holding the event - but I have interacted with both groups in different ways for many years. In the past, I went through the Level Up Initiative's mentorship program and then served as a mentor and am planning to again. I've previously written about them here. Clinical Athlete puts out podcast episodes that I've listened to and I've participated in some of their journal clubs. Both groups have loads of social media worth following and are led by super smart physical therapists who believe in educating healthcare providers. These two networks have impacted my patient care and helped me develop as a physical therapist. In my opinion, both groups are MUST FOLLOW accounts for physical therapists, strength coaches, athletic trainers, and any new grad healthcare provider - but would also be great options for sport coaches, athletes, and parents of athletes to check out! (Specific names to search for on Instagram include: @thelevelupinitiative @clinicalathlete @zakgabor.dpt @stephallen.dpt @quinn.henochdpt @jared.unbreakablestrength @rebuild_stronger - sorry if I missed anyone!) Here are some of my favorite take-aways from the Summit! (Disclaimer - this is what stood out to me, not direct quotations.)
Each day of the Summit had a theme: barbell athletes, endurance athletes, and ACL rehabilitation, with two presentations on each topic. There was key focus on the biopsychosocial approach, communication, and on case study discussion. The keynote speaker kicking off the weekend was Erik Meira, The Science PT whose talk was "The Socratic Therapist." He quoted Socrates, "What I do not know, I do not think I know," starting us off with philosophical thinking and the understanding that healthcare providers who dedicate themselves to continuous learning are simply working to be "Less Wrong" every day. None of us can really ever know for certain that what we're doing is the absolute best option for our patients, but with scientific experimentation and consideration of evidence, we can get closer to being right by increasing our knowledge. There were several moments during the course where I had the chance to think back to how my practice has evolved based on what I've learned. This was the first instance of that reflection. Erik offers his own courses, both online and in person, one of which I'm about to start after I finish ACL Study Day (there aren't enough hours in the day!). Definitely check him out. (IG: @erikmeirapt)
Day 1: The Barbell Athlete:
Presenter #1 was Stefi Cohen - a super strong woman, competitive powerlifter, and physical therapist who founded the Hybrid Performance Method and coauthored the book Back In Motion. She described her experience with a low back injury with consultations from from both Stu McGill and Greg Lehman - well known Canadian practitioners in the rehab space who have different approaches despite Greg having been a student of Stu's. Stefi shared the outcomes and her take-away understanding from those providers. She discussed that she spent four hours doing special tests with Stu McGill and ultimately was in a lot of pain for an extended period of time after her examination and that his approach to avoid certain movements and take time away from her sport didn't resonate with her - but that she appreciated his estimate on the amount of time it would take for her to get back to her previous level of competition. His timeline turned out to be fairly accurate, from what Stefi described. In contrast, she saw Greg Lehman virtually and found a rehab approach that aligned with her own beliefs and with the understanding of finding safety in movement and progressing from there. 

Presenter #2 was Quinn Henoch - founder of Clinical Athlete, competitive weight lifter, podcaster, presenter, coach, and physical therapist. Quinn's talk, "A process to help barbell sport athletes get back to those gainzzzzz" described a roadmap to coach/rehab barbell athletes. The path has bookends starting from where an athlete's current physical function is and working towards what's "done" for them. Initiation of the plan requires the physical therapist (or coach) to define their role and set expectations based on the stated goals of the athlete. Completion of training needs to be valuable to the patient - not the therapist. For some clients, "done" with a program is able to complete 1 activity or task or be able to tolerate a certain position or load. When an athlete has a specific goal in mind, we as practitioners should understand the target and guide to that. It's just like all the kids are saying these days: "Understand the assignment." It doesn't matter what I think "done" should be for my patients - if they haven't reached their goal, I've missed the mark. I definitely have fallen into this trap in the clinic where I've wanted someone to be capable of doing something that they're not interested in doing. Or, right now, I'm working with a teenager whose parent wants them to start running after an injury, but the kid wants nothing to do with running at all. Done for this patient is walking, going up and down the stairs, and participating in PE without pain. The approach has to fit the goals of the patient - not their parent and certainly not what I think matters. 

Throughout the weekend, there was an ongoing chat that allowed participants to interact with each other. I particularly enjoyed the witty banter between the powerlifters and the weightlifters throughout the weekend. As a person who likes to deadlift but who is fearful of destroying my living room if I try to snatch in my home gym, it was easy to see which side of those discussions I was on.
Day 2: The Endurance Athlete
Presenter #3: was Ellie Somers (IG: @thesisuwolf), owner of Sisu Physical Therapy and Performance, physical therapist, coach for running, strength, and businesses, and I'm proud to say, my friend, whose talk was "Communication with the Endurance Athlete." She previously worked at Seattle Children's Hospital. Ellie paired her own wit with the wisdom of Ted Lasso. Ellie also emphasized the need to have a plan with a specific purpose that is meaningful to your clients and encouraged practitioners to highlight the strengths of their patients. Too often in medicine we look at our patients and find all the things that are wrong with them. That has to change! Why can't we look at our patients and observe all the things that are great and empower them? I've emphasized this approach in my patient care and loved the quote she shared "You're not in pain because you're weak, but getting stronger can help change your pain."
Ellie also shared this article "The enduring impact of what clinicians say to people with low back pain" which I've read in the past and which is essential for young clinicians to read. It's a 2013 study from New Zealand summarizing open-ended interview questions regarding healthcare interactions and beliefs from 12 patients with acute low back pain and 11 patients with chronic low back pain. One theme was that patients had high trust in their clinicians and their beliefs were strongly influenced by what their medical providers said. However, some patients did not find their clinicians to be competent or found the medical message to be a mismatch to their beliefs and rejected what the medical providers advised. Almost subtle, a heartbreaking anecdote is a response from a study participant who shared that so many providers kept telling her back pain came from a weak core, she had an abortion because she thought she was too weak to carry and deliver a healthy baby.


Presentation #4 was Chris Johnson, owner of Zeren Physical Therapy, triathlete, presenter, running coach, and physical therapist who performed a spoken word presentation which was a unique alternative to typical presentations. Talking about running injuries, he dropped some true gems like "Tendons love tension; tendons take time (to rehab/heal)" He talked about bone stress injuries with clinical pearl: Pain with unloading the leg should evoke a high index of suspicion for a bone stress injury (BSI) and when BSI is a potential diagnosis, no progression to running should occur until walking is pain-free. Another pearl was to stop worrying so much about footwear and foot strike position with running and consider other variables such as the sound of running instead. I'll be very honest - I'm not an auditory learner, so I'm looking forward to re-reading the presentation when it gets sent out so I can further internalize the key messages and expand even further.
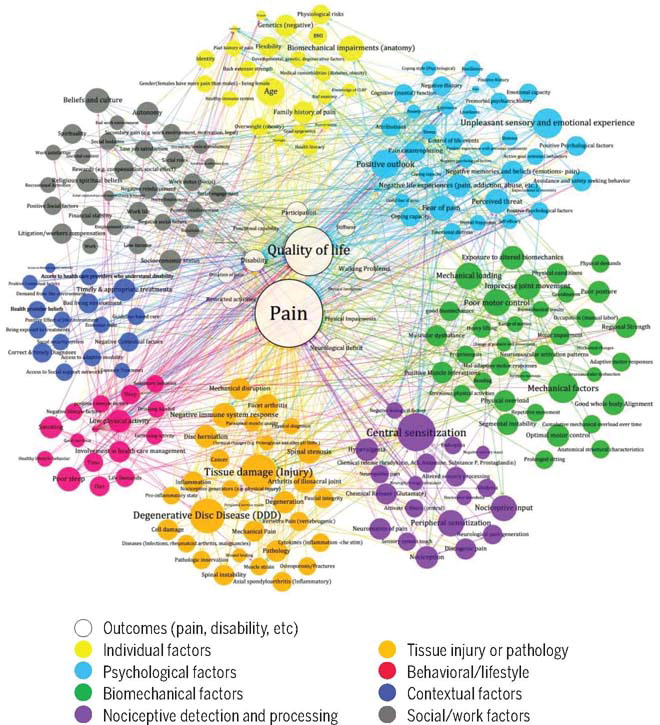
Throughout the Summit, this same image appeared three times. Isn't it nice that the presenters were so like-minded that this could happen? The picture shows contributors to low back pain (and likely applicable to most pain) from this JOSPT paper from 2019. Too hard to read? Doesn't that emphasize the point that pain is incredibly multi-factorial and the orange colored tissue-related factors are a relatively small contributor when you consider the big picture?
In my opinion, the virtual format was excellent because no travel was needed, however that does lose some of the in-person benefits like networking events and dinners. The organizers tried to combat that with a virtual Happy Hour on Day 2 where many clinicians hung out and chatted about whatever we wanted - which of course included the sports teams we support, where we're all at in the world, and lots of other interesting topics.
Day 3: ACL Injury and Rehabilitation
Presenter #5 was Derek Miles a physical therapist with Barbell Medicine who is well known for his posts about pieces of meat (representing the human body) being poked, prodded, needled, scraped, taped, or treated with other common rehab approaches to demonstrate how some of these approaches are not doing what we think they are. (IG: @derek_barbellmedicine). Derek kicked off day three's focus looking at the biopsychosocial approach for ACL injury. He reiterated the need to have a plan with rehab, outlining that the first step after an injury is to get the patient back to being a human, then an athlete, and last should be consideration for their specific sport. Walk, then run, then play basketball. How do we achieve this? Post ACL injury or surgery, there's a long list of things that people can't do. Patients should know that, but clinicians can direct their attention and focus on all the things they CAN do. Keep your athletes around their teams and with their teammates as much as possible. Send them to practice with clear understanding of what they are able to participate in. It's hard because there's a lot of discussion about what they shouldn't do, but make the injury an opportunity to learn the sport in a different way.
Early ACL rehab may be boring, but it's the foundation to the later steps and often these athletes can do more than they think they can. The ACL injury only directly impacts one limb... but there is another leg, two arms, a torso and a head that all need to continue functioning and training and should not be ignored. If your clinic doesn't have sufficient equipment to load these athletes and get them stronger, sufficient space to get them moving, and have a way to test the athlete - you probably don't have enough to adequately rehab an ACL injury. The key takeaway: LOAD HEAVIER! As Erik Meira so eloquently puts it, "It's the quad until it's not the quad." Derek said he tells his athletes to do quad sets ALL THE TIME and then, when you hate them, do 5 more, and repeat again tomorrow. No reps and sets. Just constant. I think I'll just writing 1,000,000 sets on my Medbridge HEP sheets from now on!

Presenter #6 was Laura Opstedal, owner of Build Physio in Montana who does lots of ACL Rehab and research and also previously worked at Seattle Children's Hospital. Laura reiterated Derek's points about quad strengthening and how important that is to athletic movements as well as the importance of testing athletes who have had an injured ACL prior to allowing them to return to activity. For me, one particular quote stuck out from this presentation. "Look at your entire ACL rehab program as preventing a hip strategy and forcing a knee strategy. Keep the trunk upright." I know I valued quad strength and testing before seeing this presentation, but I definitely was not doing a sufficient job avoiding the hip strategy. In fact, I've been guilty of encouraging it sometimes, but Laura addressed the inferior patella pain that some patients feel with a knee strategy that I previously was avoiding, acknowledging that sometimes these athletes are going to have a little bit of pain and we need to know when that should matter and when it's ok to continue. ACL hip strategy study. It's only been two weeks and I've already changed this in the clinic. Also encouraged were achieving passive terminal knee extension within 10 days of surgery, having at least an 80% LSI before returning to run, don't ignore calf strengthening in our patients with knee injuries, and do more open chain knee extension. There were considerations for the slow stretch shortening cycle compared to the fast stretch shortening cycle and training them separately... yup, I never thought of my rehab in those terms before, though I do have some drills I like that focus on both, the new perspective is going to make a big difference for my patients.

I definitely didn't do these presenters justice, but hopefully this "small" taste will encourage those of you who are rehab providers to start following some new clinicians and those of you who aren't in rehab who, for some reason, like to see what I have to say, hopefully learned about the complexity of pain and can gain some appreciation for the effort that any of your medical providers are putting in to maintain their licenses through continuous education and growth.
One final note: "When a measure becomes a target, it ceases to be a good measure." Using certain tests which are meant to be used to show progress and not to show culmination of progress is not the best approach. I know I often feel like my return to sport tests are the end of my rehab. This might be fine for some injuries like an ankle sprain where the athlete has been playing their sport without issue and I'm looking for a way to determine if symmetry has been restored. But in the case of an ACL injury, the RTS testing often occurs to allow the athlete to start playing their sport. This isn't good enough - and it's another chance to be less wrong tomorrow.