This is the second post in a three-part series about the San Diego Pain Summit. You can find part one here and part three here (coming soon). Part one was a look back at all the Pain Summits prior to 2023. Part three will share highlights from the February 2023 Summit.
This post summarizes what I learned from the two day pre-conference workshop with Dr. Morten Hoegh entitled "Applied Neuroscience & the Paining Person." It combines Dr. Hoegh's teachings with the tangled web my brain weaves when I try to make connections between what I'm learning and things I've thought of before. Dr. Hoegh's bio from the Pain Summit Website along with all the other 2023 Speakers' Bios highlights that he is a physiotherapist who specializes in musculoskeletal and sports physiotherapy, has a Master's of Science in Pain: Science & Society from King's College in London, and a PhD in Medicine/Pain from Aalborg University in Denmark. (Fun fact: in Denmark, they speak Danish. Don't be the dummy - like I was - who incorrectly thought they speak Dutch... Dutch is spoken in the Netherlands). Dr. Hoegh is an Associate Professor at Aalborg University and lectures around the world. He also provides patient care, which I think elevates his ability to teach to practitioners, because he understands how to apply it to the people we're working with. If you're interested in seeing his publications and learning more about his pain research, his Aalborg University Bio includes links to those. He also offers a Course on PhysioNetwork called "Pain: A Guide for Clinicians."
 |
| Morten Hoegh: humanist, skeptic, pragmatist |
Skeptic: "a person inclined to question or doubt accepted opinions." How self aware to know you're like this. I want to question my own beliefs and critically analyze things I'm learning rather than believe on first hearing. Perhaps I am now a wannabe skeptic. I think skepticism makes for improved clinical reasoning and evidence-based practice, supporting the ability to critique and seek alternative solutions. It's interesting to see how Dr. Hoegh exhibits his skepticism throughout his talk... with statements that really make you question your own beliefs. I wonder who else would proudly call themself a skeptic.
Pragmatic: "dealing with things sensibly and realistically in a way that is based on practical rather than theoretical considerations." Dr. Hoegh spent time discussing how most (all?) theories are wrong AND how they can also be useful, but if you're applying a theory, you need to recognize the limitations of where the theory can be appropriately applied. If you do something and it works, you're likely to keep doing it, even if it doesn't always work. In an effort to learn more about theories, I found this article that I found interesting discussing the difference between Scientific Theories and the use of the word theory in everyday practice. It states, "A scientific theory is accepted as a scientific truth, supported by evidence collected by many scientists. Lots of data has been collected to support theories, and no data has been identified to prove theories incorrect. That does not necessarily mean that evidence does not exist against a theory does not exist, it simply means that evidence has yet to be identified." I actually think Dr. Hoegh is a philosopher, but perhaps that's too theoretical for his liking.

It would be wrong of me to share a play by play of Dr. Hoegh's course because I will not do it justice and he gives lectures around the world worth hearing directly from him. Instead, I'll share the big picture take-away pieces about the biopsychosocial model, the classifications of pain, and peripheral and central sensitization. I won't touch upon descending modulation because - even though it was part of the course - I still don't understand it well enough to describe to another person. More for me to study at a later time!
Medical Models:
Looking through the history of medicine, illness has always been connected to a specific cause. This makes it much more difficult in current times when clinicians can't identify an underlying cause of a patient's illness or pain. The evolution of Medical Models helps us to understand where we've been - where we are now - and what's still missing.
As far back as medicine can be studied, an evil spirit or demon was thought to cause pain or illness in some religions and cultures. There was a clear separation between the body and the soul (dualism) and healing was conducted through Shaman who drove away the evil spirits to restore the body. I read this article "Judeo-Christian Concepts Related to Psychiatry," for more details, opening my eyes to the potential influences of religion on medicine and health. So, in the Beginning, there was a cause - evil spirits or sin - underlying the effect of pain or illness. With development of improved science and medicine, beliefs that other things - like bacteria or cells caused illness or that tissue damage caused pain - continued to evolve. This cause/effect relationship is a feature of the Biomedical Model and is pervasive for those who believe that physical health is separate from mental health. (I do not believe this and have previously written about that here.)
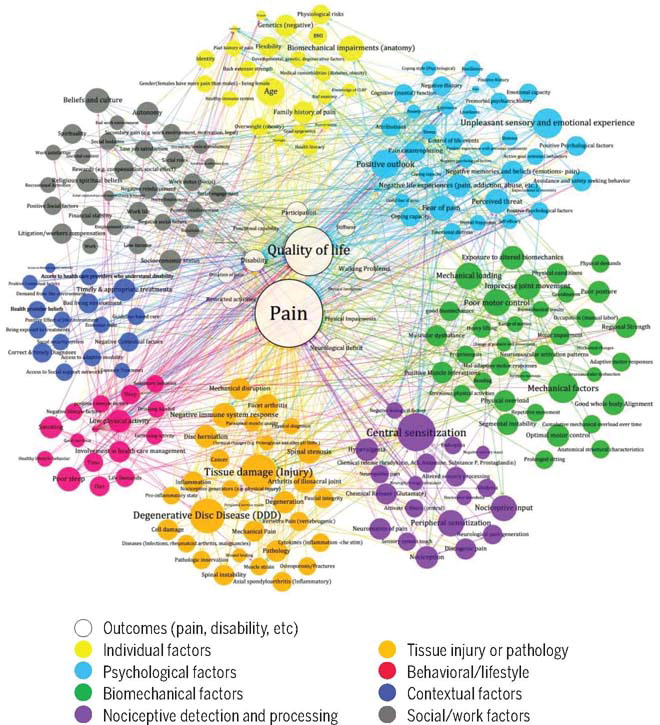
The Biomedical Model is a theory in which biological issues (think back to biology classes: cells, anatomy and physiology) are the underlying cause of disease. But as we know now, pain is far too complex for this reductionist thinking: "the practice of analyzing and describing a complex phenomenon in terms of phenomena that are held to represent a simpler or more fundamental level, especially when this is said to provide a sufficient explanation." Is it possible that sometimes a tissue injury results in pain for a human? I believe it is - however there are multiple factors that need to be considered in addition to the tissue injury that impact the individual's pain experience. The same tissue injury in multiple people will not be experienced in the same way. Pain - and illness - require broader thinking to understand, evaluate, and treat. In 1977, George Engel wrote his landmark paper challenging the Biomedical Model and naming the Biopsychosocial Model, a more integrated approach adding psychological and sociological considerations to the biological contributions. This updated model does not remove the importance of biological contributions to illness. Rather it expands the potential contributors to a broader picture that more wholly encompasses the patient's environment, beliefs, emotions, behaviors, body, and mind.
The biopsychosocial model is not meant to outline the cause of pain, though. We need to step away from the cause/effect relationship and think more about a complex interwebbing of multiple characteristics of our patients where it's not helpful to our patients to identify specific causes. We need to get more comfortable being uncomfortable and sitting with uncertainty. More and more frequently, particularly in circumstances of chronic pain, the truth is that medical providers do not know what is causing the pain. Why? BECAUSE THERE IS NOT ONE CAUSE! I think the concept that had the most impact on me from Dr. Hoegh's talk was "You have pain, period" compared to "You have pain, because..." I've now shared this conversation with two coworkers in my clinic - here's how that played out. My coworker, also a physical therapist, was evaluating a patient with a complex chronic pain diagnosis while I had documentation time so instead of writing notes, I sat in on his session. He looked at her mobility and strength, the patient's parent commented on their poor posture, an exercise program was provided that looked like it was meant to directly impact the patient's posture. Afterwards, I said to my coworker - "Do you think that patient has pain because of their posture?" and he said no! But the parent's expectation was that we needed to "correct" posture to "fix" the pain. No... the exercise program he provided looked very similar to what I would have done. It's really hard to dispute patient's and family's beliefs at the first meeting, but the language I would have used would have been to challenge the beliefs about posture as the because, explain that pain is multifactorial in nature, and get the patient moving. (Don't get me started on how much it hurts my soul when parents look at their children as if they're broken because they're experiencing pain. Your kid is not broken! Unless they have a fracture, and then, still, a piece is broken, but they're still a whole child!).
I think the development of the biopsychosocial model is a valiant attempt to reverse the reductionism of the biomedical model. Many medical providers still live in the previous biomedical model world where something happens to anatomy and they believe this causes pain. However, the biopsychosocial model encourages us to look at the human as a whole, taking into consider their biology along with their psychological and sociological environments. There are still problems with this new approach, however, if medical providers blame the biopsychosocial findings as the cause of a patient's pain. That's not how the model is intended to be used, and all too often the model is broken into it's components with each considered separately. The patient in front of you needs to be treated with consideration from all these perspectives holistically in an effort to individualize the best possible patient care. The biopsychosocial model has been broken down into separate parts for providers trying to determine if a person's pain comes from their bio, psycho, or social, when really the biopsychosocial model is not a model of pain - but rather a model of looking at illness and health for the human as a whole person who has a unique environment and history. The biomedical model is already a big mess for medicine, can we try to avoid the same disaster with the biopsychosocial model? That was a lot of philosophy for a Neuroscience Talk, wasn't it?!
International Association for the Study of Pain (IASP) Pain Classifications
Dr. Hoegh is really quite genius in teaching pain neuroscience. He's currently in the process of releasing a series called "Pain Science in Practice" through the Journal of Sports Physical Therapy JOSPT, all parts so far are less than 3 pages of digestible pieces about pain neuroscience. They're great. The course discussed the first five of these papers that have been released and more are coming soon. I highly recommend them for the new PT and the Painiacs like me to better help understand pain mechanisms.
 |
| Dr. Hoegh's Pain Classifications |
 |
| Dr. O'Connor's Pain Classification Continuum |
 |
| Tooth Fairy © Irina Akolzina |

This is the meat and potatoes. This is the part that I see in my patients, scratch my head, and wonder why it's happening for so long instead of going away. Both Peripheral and Central Sensitization are cases of the nervous system being sensitive. Things that wouldn't normally hurt, now might - or things that would hurt before, hurt more than they previously did.
The Central Nervous System includes the brain and spinal cord - so the underlying mechanisms of Central Sensitization occur there. The Peripheral Nervous System is the rest of the nervous system, all the nerves that come out from the spinal cord and provide sensation and movement to the rest of the body.
 |
| JOSPT Pain Science in Practice #3 Peripheral Sensitization |
Peripheral Sensitization is sensitive to heat where central sensitization is not - so if a person was complaining of pain and you applied heat, worsening symptoms could indicate peripheral sensitization. At the time of an injury, sensitization is normal! You broke your leg - a sensitive leg reminds you not to put weight on it! The picture shows peripheral sensitization where an injury (far left) results in inflammation (all the little balls) and that inflammation is a bunch of chemicals that attach to different receptors on the nerve (blue part on the right). If the inflammation continues to occur, the receptors on the nerve get more sensitive to them. So in a nociceptive pain situation, the injury occurs, inflammation happens, and then the tissue heals and inflammation stops. In a nociplastic situation, the tissue heals, but for some reason, the sensitive receptors remain sensitive. This may be related to the mast cells (purple blob) or the immune cells (brown blob) which also give out inflammatory chemicals.
 |
 |
| Me with Dr. Morten Hoegh |
A final thought about therapeutic alliance. As always. I've written about therapeutic alliance in several blog posts, this one probably being my favorite. Dr. Hoegh wrapped up his two-day talk with great reminders about the importance of the patient-clinician relationship. It truly does not matter how much pain neuroscience you know if you can't connect with your patients. Can you empower your patient, even when they're in pain, to finish a session with an "I did it!" feeling? Can you help create situations where they meet success after success after success and stop a potentially perpetual cycle of failures? Can you find a topic to talk about so your patient who has depression and is sad has a moment of laughter or joy so that there is positivity breaking up the negativity? Empowering your patients can be a powerful behavior change tool to get them moving in new ways to change their pain experience. I once had a patient who was in treatment for CPRS and had spent months in his bed. He was improving very slowly, but after a family discussion to get some new bedding and a new poster and rearrange the furniture in his room, things got dramatically better. He had a new environment, a change of habits, and something that brought him excitement that previously was part of his negative state. Would I say that this change caused his pain to improve? No. He had pain, period. Not pain, because his room was part of the problem. I'm really excited to move away from pain, because. I hope you'll join me. Thank you, Morten!